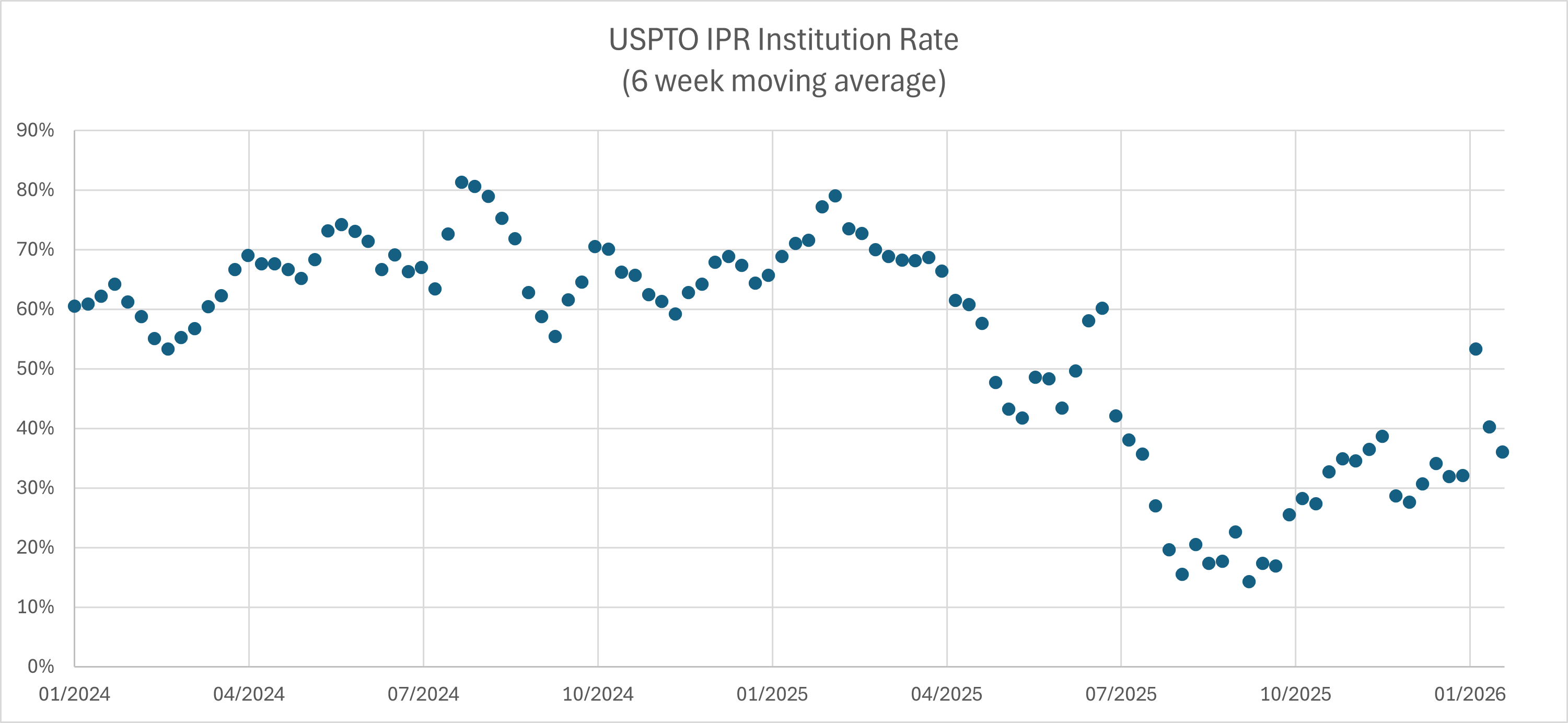
IPR institution rates under Director John Squires have begun to climb. My tracking data shows the six-week moving average rising from lows around 15% in August and September 2025 to somewhere in the range of 35-55% by late December 2025 and into January 2026. The rebound remains far below the historic average of roughly 67% that prevailed before Acting Director Coke Morgan Stewart began centralizing discretionary denial authority followed by Director Squires assumption of personal control of all institution decisions in October 2025.
Still, the uptick signals something meaningful: the IPR system is not dead, and a discernible framework for institution has begun to emerge from what initially appeared to be an era of blanket denials. The patterns in recent grants reveal that Director Squires is operating with something resembling an equitable framework that requires petitioners to go beyond the statutory "reasonable likelihood" threshold to encompass broader considerations of fairness and systemic efficiency. The USPTO's recent designation of numerous institution decisions as precedential or informative in early January 2026 provides additional clarity about the principles the Office considers settled enough to guide future practice.
Google won today's eligibility case with an affirmance that US7679637 is ineligible. For me, the following are the two most interesting aspects of the decision:
Tu Quoque Rejected: The patent owner argued that Google's own video conferencing patents use similar "functional claiming" techniques, and therefore Google must believe such claims are patent-eligible. The Federal Circuit rejected this hypocrisy-style argument, holding that the eligibility of Google's patents "is not before us and has no bearing on our analysis."
Where Does Functional Claiming Fit? At oral argument, Chief Judge Moore candidly admitted doctrinal uncertainty: "Is this result-oriented functional claiming problem . . . a Step 1 issue or a Step 2 issue? I'll be honest with you, I don't always know where that line is." The opinion resolves this by treating functional claiming as part of the Step 1 "directed to" inquiry.
Comcast has asked the Supreme Court to review whether the Federal Circuit violated fundamental principles of party presentation when it held that a district court "legally erred" by not construing patent claim terms that the patentee had successfully argued required no construction. The petition in Comcast Cable Communications, LLC v. WhereverTV, Inc., No. 25-___ (filed Jan. 2026), frames the issue as a conflict between the Federal Circuit's O2 Micro doctrine and the Supreme Court's recent reaffirmations of adversarial limits on judicial power. At its core, the case presents a doctrinally neutral question: when a party deliberately waives an issue before the district court, can the appellate court override that strategic choice and decide the issue anyway?
The Federal Circuit has a new expert witness case -- this time siding with the patentee and finding that two experts were improperly excluded mid-trial. But, the case includes a sharp dissent over where to draw the line between a court's Daubert gatekeeping function and the jury's role as factfinder. Barry v. DePuy Synthes Companies, No. 2023-2226 (Fed. Cir. Jan. 20, 2026).
In the case, the experts had presented testimony that strayed somewhat from the court's claim construction and also included survey results using questionable methodology. Writing for the majority, Judge Stark concluded that this testimony was (1) permissible applications of the court's claim construction and (2) that methodological criticisms went to evidentiary weight rather than admissibility. Judge Prost dissented, warning that the majority's approach "contravenes the principles embraced in EcoFactor and the 2023 amendments" to Federal Rule of Evidence 702 and "will undermine district courts' abilities to exercise their important gatekeeping function."
The dispute in this case highlights a conceptual tension in how we think about expert testimony standards. All testimony must clear a basic relevance threshold to be admissible. At the other end of the spectrum, we have a higher standard for actually carrying the burden of proof and sustaining a verdict. Expert testimony occupies middle ground. Rule 702 and Daubert impose reliability requirements that exceed ordinary admissibility standards, recognizing that experts wield particular influence over juries. But, where exactly expert testimony sits on this spectrum (and who decides) is the central tension between the majority and dissent.
I only recently started using mobile check deposits. I don't get very many checks these days, but when I do it is a real pain to drag myself to the the bank to deposit -- particularly because I don't carry my ATM card with me. Great convenience -- and also a great patent story.
USAA is a financial services association cooperatively owned by U.S. military members, veterans, and their families. Because USAA serves military families whether stationed at home or deployed overseas to places like Iraq and Afghanistan, it does not operate a traditional branch network. This created a persistent problem: how could USAA members deposit checks when stationed far from any bank? Starting around 2005, a team at USAA began researching technology that would allow members to deposit checks from anywhere in the world using devices they already owned. The challenge was formidable: as of the 2006 priority date, the banking industry conventional wisdom was that specialized check-scanning equipment was the only way to reliably capture check images meeting the technical requirements for remote deposit under the Check 21 Act. USAA's engineers developed a system using a downloaded mobile app to assist customers in capturing compliant check images without specialized equipment, launching Deposit@Mobile in 2009 as the first mobile check deposit service offered by any U.S. bank. Within a month, it became the number one financial app in the Apple app store, with members depositing over 1.5 million checks in the first year.
The Supreme Court has granted certiorari in Hikma Pharmaceuticals USA Inc. v. Amarin Pharma, Inc., No. 24-889, likely the only patent case this term. In doing so, it takes up the question of whether a generic drug manufacturer can face induced infringement liability when it markets a product using a "skinny label" that fully carves out patented uses.
The case presents the Court's first opportunity to directly address the intersection of patent inducement doctrine and the Hatch-Waxman Act's section viii carve-out provisions, which allow generics to obtain FDA approval for non-patented indications while omitting still-patented methods of use from their labeling. Hikma's generic version of Amarin's Vascepa (icosapent ethyl) received FDA approval only for severe hypertriglyceridemia, with the more valuable cardiovascular risk reduction indication carved out pursuant to section viii.
The Federal Circuit nonetheless permitted Amarin's inducement claims to proceed, finding that Hikma's marketing statements and press releases, combined with its label, plausibly alleged that Hikma encouraged doctors to prescribe the generic for the patented cardiovascular use.
The grant follows the Solicitor General's December 2025 brief recommending review, which argued that the Federal Circuit's approach threatens to undermine Congress's purpose in creating the skinny-label pathway.
In my view, the generic Hikma is likely to win before the Supreme Court. But, the court is unlikely to create an express skinny-label exception. Rather, I believe the court will decide the case based upon traditional inducement liability doctrine. That means that the resolution will shape not only pharmaceutical competition but potentially the scope of inducement liability across all patent-intensive industries.
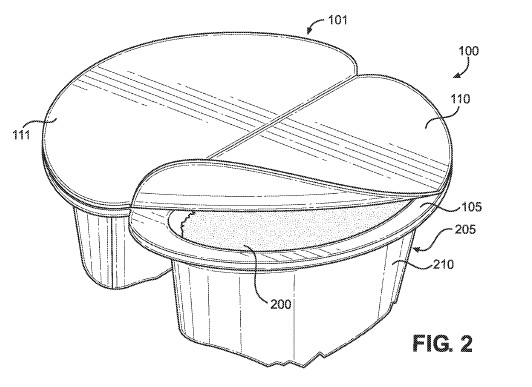
The Federal Circuit affirmed a PTAB obviousness rejection in In re Blue Buffalo Enterprises, Inc., No. 2024-1611 (Fed. Cir. Jan. 14, 2026), holding that the claim terms "configured to" and "configured for" mean "capable of" performing the recited function absent specification language suggesting a narrower construction. The nonprecedential decision, authored by Chief Judge Moore and joined by Judge Taranto and visiting District Judge Chun, rejected the applicant's argument that "configured to" should be construed as "specifically designed to" perform the claimed function. Blue Buffalo's application claimed a wet pet food packaging container with deformable sidewalls and an integrated tool portion for tenderizing food. The claim recited sidewalls "configured to be readily deformable" and the integrated tool having projections "configured for use in breaking up and/or tenderizing the food product." The Board construed both phrases as requiring only that the structures be capable of performing these functions, which allowed the Coleman prior art reference to anticipate the limitations. Blue Buffalo conceded at oral argument that it was not challenging the obviousness determination under the "capable of" construction, effectively staking its entire appeal on claim construction.
The case arrives at an apt moment to note that the law surrounding "configured to" claim language has become something of a dog's breakfast. Over the past two decades, prosecutors have increasingly deployed "configured to" as an alternative to means-plus-function language under 35 U.S.C. § 112(f), hoping to capture functional aspects of an invention without limiting claims to the structures disclosed in the specification and their equivalents. The appeal of "configured to" is that it sounds structural while still defining the invention by its functional results. But this strategy carries real risk. In addition to the categorization in this case, the court could have instead found that the language invokes § 112(f) after all.
At oral argument, Chief Judge Moore cut to the heart of the matter with a question that frames the entire dispute. After Blue Buffalo's counsel argued that "configured to" should mean "specifically designed to," Judge Moore responded:
My concern at a high level is that you're taking a product claim that has to have structural limitations and you're infusing an intent element. Intent. That the person had to design this structure with this intent in mind, as opposed to: we designed this structure without that intent, but it happens to actually do that. I feel like that's good enough because it's a product claim.
Oral Arg. at 3:06 (Chief Judge Moore). Judge Taranto pressed the point further, asking whether "configured to" could become "magic words added anywhere to have the effect that you're talking about, to add this intent element." Oral Arg. at 6:40. Judge Taranto followed up with the key problem of adding an intent element into a product claim:
You [would] have to identify either the ... defendant's designer or manufacturer, and what that entity or person was thinking about when creating this particular structure.
I wanted to add a quick update here on pending Supreme Court cases.
The court has denied cert in two cases: SurfCast v. Microsoft (25-555) (R.36 case) and Vetements v. Stewart (25-215) (international translation in trademarks). Most notably, it redistributed the skinny label case of Hikma v. Amarin (24-889) to its January 16 - a signal typically seen as increasing the likelihood of grant. Several other patent cases remain in various stages of briefing, with one presenting an unusual procedural posture.
Hikma's redistribution follows the traditional trajectory toward certiorari. The case asks whether a generic drug manufacturer that fully carves out patented uses from its FDA-approved label can face induced infringement liability based on marketing statements and publicly available information about the branded product. The Solicitor General filed a supportive brief in December 2025 recommending that the Court grant review, arguing that the Federal Circuit's approach creates uncertainty about the scope of protection the Hatch-Waxman framework provides for skinny-label generics. See Dennis Crouch, Label-Plus Liability: The Government Warns the Federal Circuit Misread Hatch-Waxman, Patently-O (Dec. 2025). Cases receiving favorable CVSG responses historically have high grant rates, and redistribution to a second conference further increases the odds.
Director Squires has designated as precedential a new decision restricting parallel IPR petition practice at the PTAB. In PacifiCorp v. Birchtech Corp., IPR2025-00687, Paper 40 (P.T.A.B. Jan. 12, 2026), the Director vacated institution decisions in four inter partes review proceedings where petitioners had filed two petitions against each of two patents. The petitions divided their invalidity arguments according to two separate invalidity theories: (a) pre-priority-date prior art and (b) intervening art that required challenging the patent's priority claim. Director Squires held that this parallel-petition strategy was not justified because petitioners had ample room in each petition to present alternative arguments. The decision follows and cites Acting Director Stewart's June 2025 decision in CrowdStrike, Inc. v. GoSecure, Inc., IPR2025-00068, Paper 25 (P.T.A.B. June 25, 2025) (informative), which similarly vacated dual institutions, but the precedential designation of PacifiCorp nominally converts this guidance into binding Board practice.
A major caveat: the precedential status of this decision does not actually constrain USPTO institution practice since institution decisions are no longer decided by the Board but rather by Dir. Squires himself. To borrow from James Madison in Federalist No. 48, this designation is a mere 'parchment barrier.' It provides the appearance of structural constraint, but the Director holds the power to both legislate the rules and decide the cases. And, as the government recently argued before the Federal Circuit, the Director is not bound by PTAB precedent. One might recall the apocryphal boast attributed to Louis XIV: "L'État, c'est moi." Designating a decision as binding on "the Board" is a semantic distinction without a difference when the Director is the entire patent office; or as it were, "L'Office, c'est moi."
Second Decision: Director Squires has also issued an informative decision in Top Glory Trading Group Inc. v. Cole Haan LLC, IPR2025-01395, Paper 18 (P.T.A.B. Jan. 12, 2026), refusing discretionary denial in a design patent case. PetitionerThe Patentee had argued that settled expectations should shield the patent from review, but the Director rejected this argument based upon the unique design patent circumstances. In particular, the Federal Circuit's 2024 decision in LKQ Corp. v. GM Global Technology Operations LLC, 102 F.4th 1280 (Fed. Cir. 2024), fundamentally changed design patent obviousness doctrine and thus removed assurances that the patent was properly examined for obviousness.
Notably, the decision confirms that settled expectations generally remains an important discretionary consideration under current USPTO policy, but clarifies that a significant change in law can overcome reliance-based arguments.
An interesting international patent issue is stirring regarding when it is appropriate for one nation's courts to pass judgment on patents issued in other countries. A key pending case involves Onesta IP, who has obtained a number of U.S. and foreign GPU-related patents from AMD. Onesta argues that BMW's vehicles equipped with Qualcomm Snapdragon chips in their infotainment head units infringe the patents. However, rather than suing in U.S. Court, Onesta sued in a Munich regional court, asserting infringement of a European patent alongside two U.S. patents (Nos. 8,854,381 and 8,443,209). That German case is ongoing, but BMW responded by filing a declaratory judgment action in the Western District of Texas, and Judge Alan D. Albright promptly granted an ex parte temporary restraining order preventing Onesta from seeking an anti-anti-suit injunction in the German proceedings. BMW v. Onesta IP, LLC, No. 6:25-cv-00581 (W.D. Tex. Dec. 16, 2025). That TRO was extended on December 30, 2025, with a preliminary injunction hearing scheduled for January 13, 2026. This post looks at the European jurisdictional shift that enabled Onesta's strategy, BMW's defensive response through the U.S. anti-suit injunction, and whether this changed international landscape should prompt reconsideration of the limits U.S. courts have placed on their own authority to adjudicate foreign patent claims.
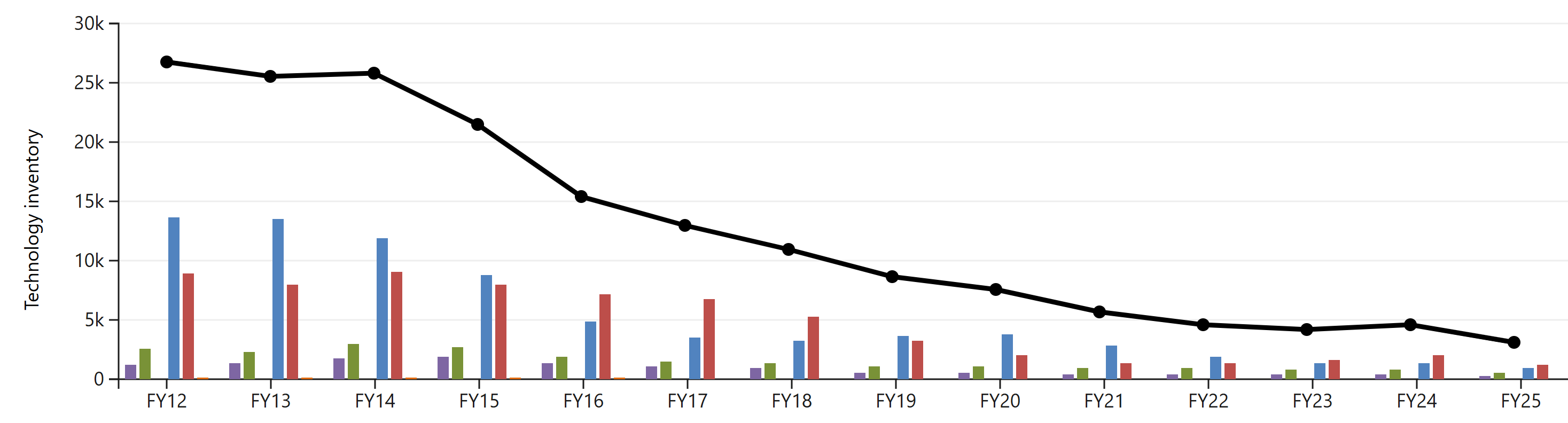
The PTAB is likely to undergo a dramatic transformation in 2026 based upon the convergence of two parallel developments. (1) The ex parte appeal inventory has plummeted from approximately 27,000 pending appeals in FY2012 to under 3,000 today, with the trajectory suggesting near-zero inventory within months. (2) Simultaneously, Director John Squires has effectively shut down inter partes review through aggressive use of institution denials. The combination means the PTAB's role is shrinking on both fronts, raising fundamental questions about what happens to an institution built for a workload that no longer exists.
The workforce implications are stark. Before President Trump's inauguration, the PTAB employed approximately 230 Administrative Patent Judges plus roughly 120 support staff. That number has already dropped to fewer than 200 APJs through DOGE attrition and early retirement incentives. But I believe this reduced headcount is still dramatically oversized for the emerging workload.
Patently-O remains a very small operation, but we’ve added an operations manager to help keep things running smoothly. If you have subscription questions, login issues, billing matters, or other administrative needs, you can now reach out directly to discover@patentlyo.com.
This should mean faster responses on the operational side while I stay focused on the content.
This week I'm delivering a talk on Patent Law issues from 2025. The year has been defined by institutional upheaval, including the the effective shutdown of new inter partes review institutions and a USPTO willing to fill doctrinal voids that Congress and the courts have left open. The following are seven issues that I think deserve ongoing consideration.
In Technology in Ariscale, LLC v. Razer USA Ltd., No. 2024-1657 (Fed. Cir. Jan. 6, 2026), the Federal Circuit affirmed the district court's judgment that claims 1 and 14 of U.S. Patent No. 8,139,652 are invalid under 35 U.S.C. § 101 for claiming patent-ineligible subject matter. The nonprecedential decision, authored by Judge Cunningham, illustrates continuing difficulty patentees face when attempting to frame mathematical signal processing operations as concrete technological improvements. The case also demonstrates how a patent's own specification can undermine eligibility arguments in situations where the disclosed benefits do not map directly to the actual claim language.
The Federal Circuit heard oral argument today in Apple Inc. v. Squires, 24-1864, a long-running challenge to the USPTO's Fintiv discretionary denial framework. Apple, Cisco, Google, and Intel argue that the NHK-Fintiv rule should have been adopted through notice-and-comment rulemaking under the Administrative Procedure Act (APA) rather than through precedential Board designations. The case presents a narrow but consequential question: when the Director instructs the PTAB how to exercise delegated institution authority, does that instruction constitute a "substantive rule" requiring APA procedures, or merely a "general statement of policy" that the agency may adopt without public input? The panel of Judges Lourie, Taranto, and Chen pressed both sides on whether a rule binding only on the Board triggers notice-and-comment requirements when the Director remains free to deviate from it entirely.
This is an important case, but some amount of practical obsolescence based upon the dramatic 2025 changes to institution practice. Still, as I explain at the end of the post, a strong win for the government could have a much larger impact on how the USPTO operates within the Federal regulatory framework.
Things look pretty thin. The Supreme Court has not granted certiorari in any patent cases this term and only four are still pending before the Court. But the ones that are pending include some important questions. Of the four, one stands out as the most likely candidate for certiorari: Hikma Pharmaceuticals v. Amarin Pharma, a Hatch-Waxman induced infringement case that received a supportive call-for-the-views-of-the-Solicitor-General (CVSG) response. The January 9, 2026 conference also includes one other patent cases along with one trademark dispute. A two additional patent cases remain in briefing: Lynk Labs v. Samsung and Agilent v. Synthego.
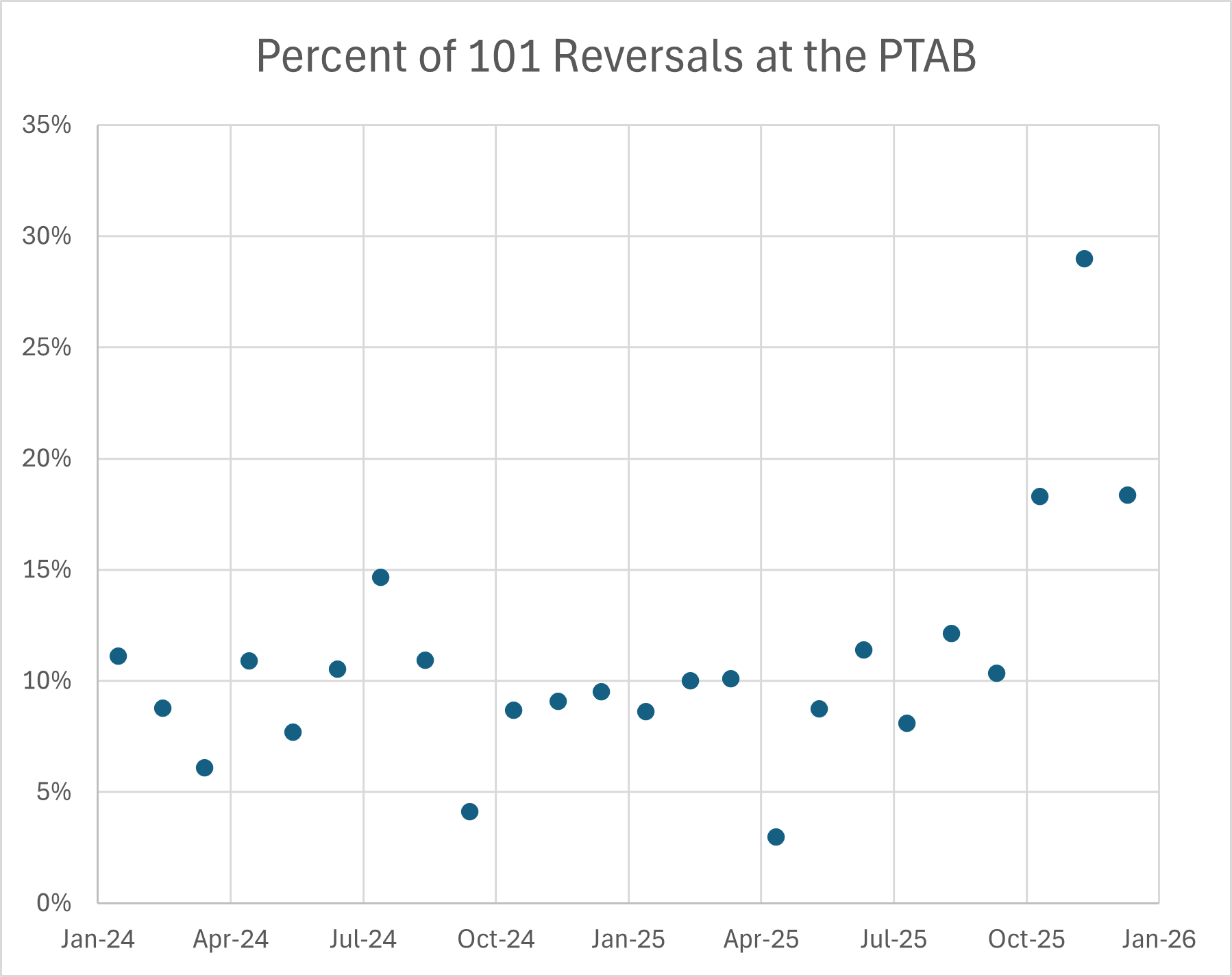
The Patent Trial and Appeal Board (PTAB) has doubled its rate of reversing Section 101 rejections since Director John Squires took office, according to my new analysis of ex parte appeal decisions involving eligibility challenges from 2024 and 2025. The reversal rate, which hovered between 8% and 12% for most of 2024 and early 2025, jumped to 18% in October 2025 and spiked to 29% in November. A recent rehearing decision in Ex parte Mercer, Appeal 2024-002371 (PTAB Oct. 31, 2025), illustrates one aspect of the Board's new approach: demanding evidentiary support for findings that claimed elements are "well-understood, routine, conventional activity" under Alice step two.
The chart above shows the percentage of Section 101 rejections reversed by the Board (without a new ground of rejection) in ex parte appeals, by month. As I discussed in October, the Board's Section 101 reversal rate began climbing shortly after Director Squires took office. Dennis Crouch, PTAB Responds to New Director with Increased § 101 Reversals, Patently-O (Oct. 2025). The trend has accelerated. The November 2025 reversal rate of 29% represents nearly a threefold increase from the rates that prevailed through most of 2024.
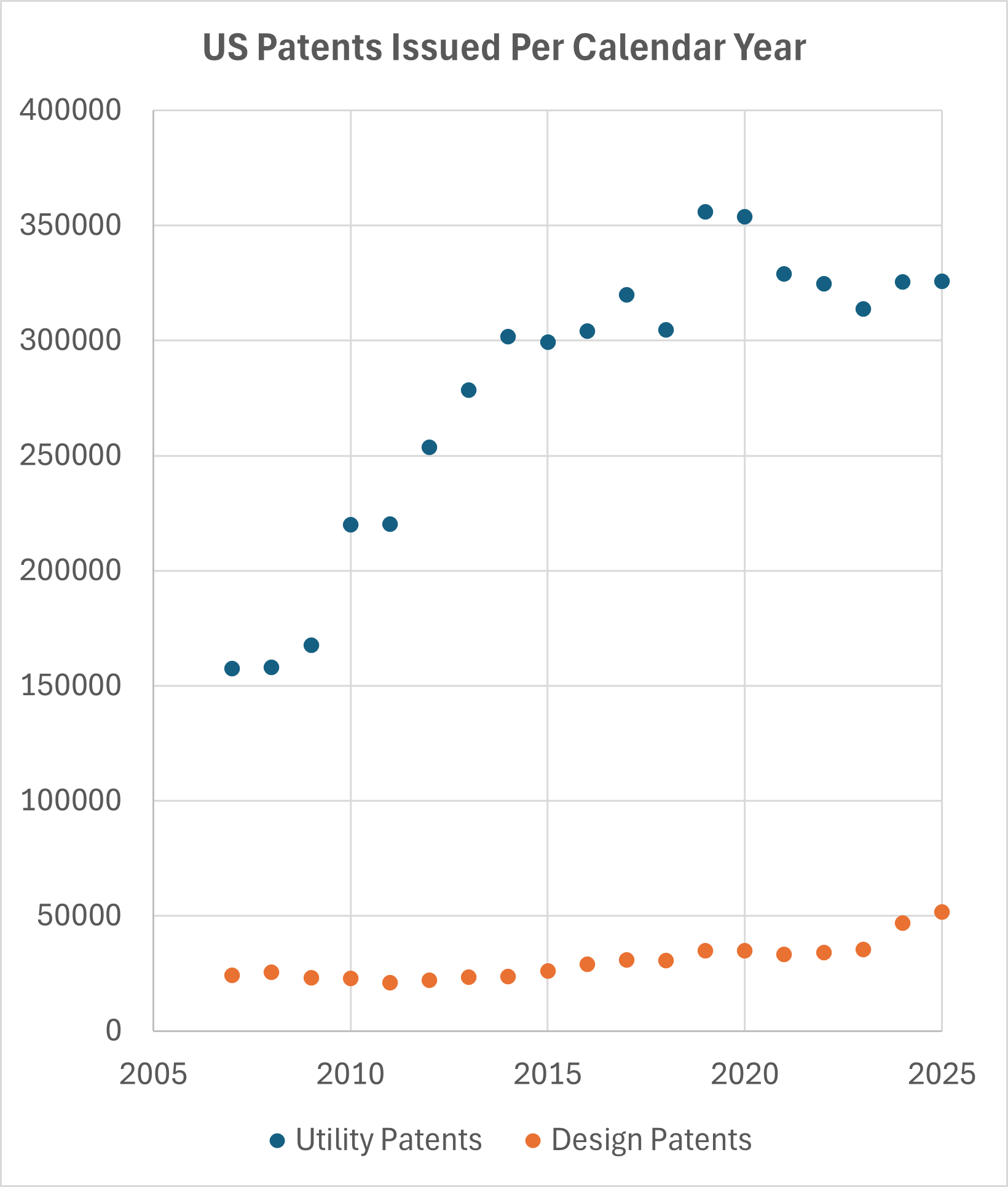
The USPTO issued ~325,800 utility patents in calendar year 2025, a figure virtually unchanged from the ~325,600 issued in 2024. This stability marks another year in what has become a post-pandemic plateau for utility patent issuances, with annual totals hovering around this mark since 2021. The days of dramatic year-over-year growth appear to be behind us, at least for now. Over the past two years, allowance rates have also remained virtually unchanged.
Design patents tell a different story. The 52k design patents issued in 2025 represent a 10% increase over 2024 and mark the highest annual total on record. This growth reflects the continued global importance of design protection, with non-U.S. applicants increasingly seeking design patent rights in the American market. The design patent surge stands in contrast to the flat utility numbers and suggests that different forces are shaping these two branches of patent protection.
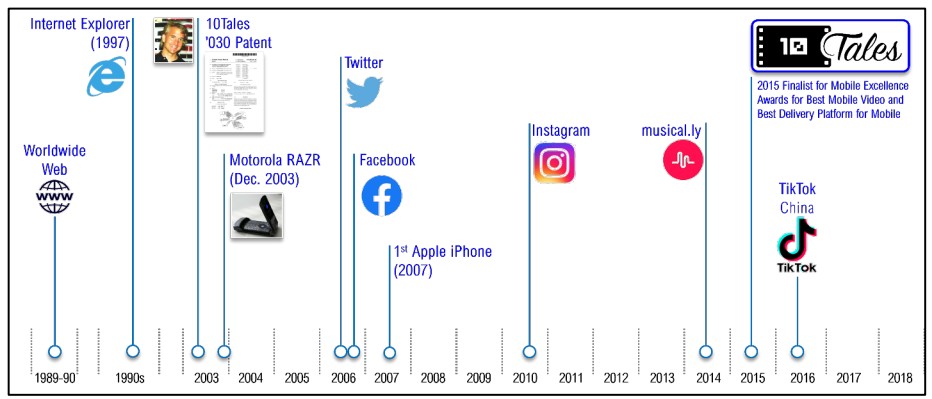
I'm watching the pending eligibility appeal in 10Tales, Inc. v. TikTok Inc., No. 2024-1792 (Fed. Cir.). The appellant is challenging a Northern District of California's grant of judgment on the pleadings finding claim 1 of U.S. Patent No. 8,856,030 directed to the abstract idea of "presenting personalized content to a user based on information about the user." In some ways, the case presents a straightforward application of the Court's targeted-content precedents, but the patent's timing raises interesting questions about how we should evaluate innovation with the benefit of hindsight.
The '030 patent, filed in April 2003, is directed to a system that retrieves information about users from their interactions in online communities and uses that information to select and substitute digital media assets, creating personalized content displays. The district court held that claim 1 fails both steps of the Alice framework: at step one, the claim is directed to the abstract idea of personalizing content; at step two, the claim elements are conventional computer functions that do not supply an inventive concept. On appeal, 10Tales argues that the district court over-generalized the claim at step one and failed to recognize that retrieving "user social network information" from external sources and performing "rule based substitution" of digital assets constituted inventive features at step two.
The Federal Circuit has affirmed an exceptional case finding and attorney fee award against Ortiz & Associates in its patent infringement action against Vizio. Ortiz & Associates Consulting, LLC v. Vizio, Inc., No. 2024-1783 (Fed. Cir. Dec. 17, 2025) (nonprecedential). Writing for the panel, Judge Bryson found no abuse of discretion in the district court's determination that the case "stands out from others" under Octane Fitness, LLC v. ICON Health & Fitness, Inc., 572 U.S. 545 (2014).
The decision also raises (but doesn't decide) an underdeveloped issue involving NPE litigation and patent marking.
The Patent Marking Statute
Many of us are familiar with products marked as PATENTED and then listing the patent number. Patent marking allows a patentee to provide constructive notice and thus permits collection of back damages for up to six years. Under 35 U.S.C. 287(a), "[i]n the event of failure so to mark, no damages shall be recovered by the patentee in any action for infringement, except on proof that the infringer was notified of the infringement and continued to infringe thereafter."
A huge caveat to the rule is that back damages are permitted without notice in situations where there is no product to be marked. This is typically the case for non-practicing entity (NPE) litigation where the plaintiff's key asset is the patent. But, the NPE status goes away once the patent is licensed, which is the common result of patent litigation settlement.